
Safety science has gone through six distinct paradigm shifts since the 1920s. Most organisations are still operating in the wrong one.
👋 Hello, Lucas Domingues here and welcome to the 5th edition of Safety 4.0 Insights in 2026. As AI in EHS content floods the internet, true signal is becoming rare. This newsletter is where we keep it real: human, SafetyTech clarity, and practical AI for EHS leaders. Thanks for helping make it a leading publication.
🎓 Now is a great time to learn and upskill in AI, safetytech and digital transformation. Here's how I can help you:
- Applications are OPEN for the May Cohort (starting on May 5th) of my Safety 4.0 Accelerator (IOSH approved and CPD certified). A global 4-week on-line interative programme designed by and for senior EHS Leaders to build digital fluency and readiness in the digital age. [special discount for groups or in company].
Let's go 🚀
In 1931, Herbert Heinrich published a book (Industrial Accident Prevention) that would define workplace safety for the next decades. Its core claim: most accidents are caused by unsafe acts of workers. Control the worker, control the accident (in 2026, many organisations still operates like this 🫤)
This edition traces six eras of safety thinking: from the accident-prone worker of the 1920s to the AI-powered risk systems of today, and of course, how you should respond to this shift.
ERA 1 · PRE-1931
Survival of the Careful
Before formal safety science, accidents were treated as individual failures of careless workers. In the US, law shielded employers from most liability. The 1911 Triangle Shirtwaist fire which killed 146 workers trapped behind locked exits catalysed the first wave of US labour safety legislation, but left the underlying logic intact.

A lunch atop a skyscraper is a famous 1932 photograph showing 11 workers eating lunch on a steel beam.
ERA 2 · 1931–1969
Heinrich's Dominos: The Engineering of Blame
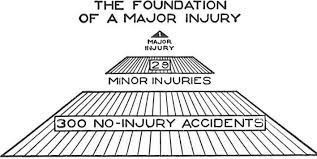
Heinrich's Domino Theory framed accidents as a chain of five sequential factors, with the "unsafe act" as the critical domino to remove. He also introduced the Safety Pyramid: one major injury for every 29 minor injuries and 300 near-misses implying that suppressing near-misses would suppress serious accidents.
Heinrich's analysis concluded that 88% of industrial accidents resulted from unsafe acts of workers, 10% from unsafe conditions, and 2% from unpreventable causes.
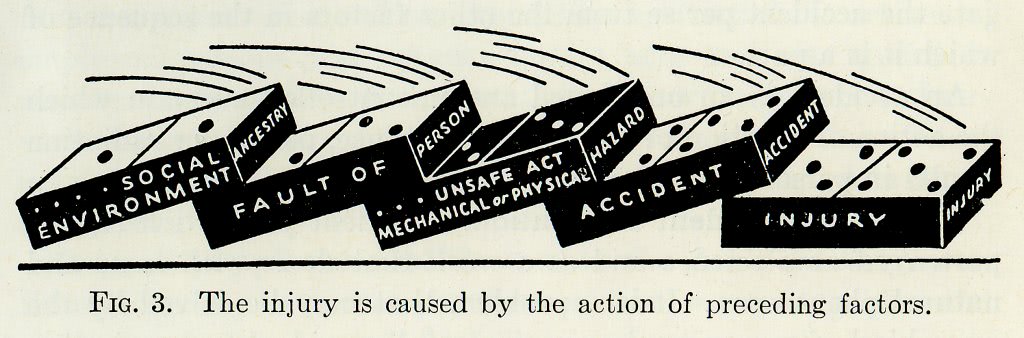
Henrich's domino accident causation
Bird's 1969 study at the Insurance Company of North America analysed 1.7 million incident reports across 297 companies and revised the ratio to 1:10:30:600, adding property damage as a distinct category.
Both models embedded a worker-centric view that would shape safety practice for decades. Despite of the criticism (mine included), such studies have made significant contributions to workplace safety science over the years.
ERA 3 · 1970–1986
The Regulatory Era: Compliance as Safety
The US Occupational Safety and Health Act (1970)and the UK's Health and Safety at Work Act (1974) created statutory duties and enforceable standards. Fatality rates declined across industrialised economies. But the default response to regulation was procedural: policies, training records, documented risk assessments with completion treated as evidence of control.
Key Pattern: Regulation created accountability, but also the conditions for safety-as-paperwork — where documentation of risk management became the primary evidence of risk management.
The hierarchy of controls existed in theory, but organisations gravitated to the cheapest options: administrative controls and PPE, rather than elimination or engineering solutions.
ERA 4 · 1986–2000
Systems Thinking: Reason's Swiss Cheese
The disasters of the 1980s Chernobyl (1986), Herald of Free Enterprise (1987), Piper Alpha (1988) and others discredited the individual-blame narrative. These were systems failures. James Reason's Swiss Cheese Model (1990) reframed accidents as the alignment of latent organisational conditions with active failures at the frontline.
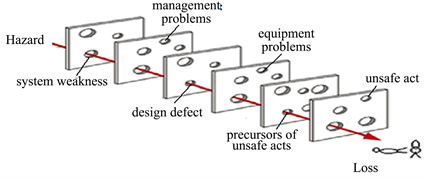
Reason's Core Argument: Addressing individual errors without changing the underlying system is like removing symptoms without treating the disease. The most powerful interventions target latent organisational conditions — not frontline behaviour.
ERA 5 · 2001–2015
Safety Differently: Understanding Work
By the 2000s, major accident rates in some industries had plateaued despite strong management systems. Sidney Dekker's Field Guide (2006) shifted the investigator's question from "why did people fail to follow the system?" to "why did their actions make sense at the time?"
Erik Hollnagel's Safety-II (2015) added a second shift: safety is not only the absence of failure, but the presence of successful adaptation. Work-as-imagined (procedures, assumptions) differs systematically from work-as-done — and organisations monitoring only the former are operating blind.
ERA 6 · 2016–PRESENT
Safety 4.0: Real-Time Intelligence
Safety 4.0 applies IoT sensors, AI analytics, wearables, and digital twins to occupational health and safety, enabling continuous risk monitoring at scale. Used well, it provides the infrastructure to implement earlier paradigms properly: data for systems thinking, visibility for Safety-II. Used badly, it becomes AI surveillance grafted onto a blame culture amplifying old problems at new speed.
This is not a passing trend. The EU's Strategic Framework on Health and Safety at Work 2021–2027 names the digital transition as one of three strategic priorities for worker safety and health. IoT sensor costs are falling, AI accountability is entering law, and organisations are rebuilding how operational risk is measured. The infrastructure of safety is being rebuilt whether practitioners participate in it or not.
Why Practitioners Can't Sit This One Out: If safety professionals aren't in the room when these tools are specified, procured, and deployed, the default user becomes HR, IT, or Operations and tools get shaped to their objectives, not safety's. Learning Safety 4.0 isn't about becoming an engineer. It's about understanding these tools well enough to shape how they're deployed, so they serve hazard elimination and engineering controls, not just surveillance of workers.
The Era Diagnostic
Which era is your organisation actually operating in?
Most organisations are not in a single era; they are a patchwork. The goal is not to reach Era 6, but to understand where the dominant logic of your safety programme sits, and where that creates risk. Use this in post-incident reviews, culture assessments, or leadership conversations.

What to Do With This
The most common pattern I see: Era 6 technology budgets running on Era 3 safety cultures. Sensors, dashboards, and AI-powered reporting sitting on top of blame-oriented investigations and culture. Each era contributed something real. The question isn't which is "best" but whether your organisation's dominant logic matches the complexity of the hazards you face.
Practitioner Action: Take one recent incident or near-miss investigation report. Apply the diagnostic above to its conclusions and recommendations. Which era does the investigation's logic belong to? That is your current operating paradigm regardless of what your safety policy says.
The lever isn't more technology or more procedures. It's the quality of the questions your investigation process asks. That is where paradigm shifts become practical.
🙏 Thank you for reading!
Have a great day, stay safe, stay ahead.
Lucas
References
- Aldrich, M. (1997). Safety First: Technology, Labor, and Business in the Building of American Work Safety, 1870–1939. Johns Hopkins University Press.
- Von Drehle, D. (2003). Triangle: The Fire That Changed America. Atlantic Monthly Press.
- Heinrich, H.W. (1931). Industrial Accident Prevention: A Scientific Approach. McGraw-Hill.
- Bird, F.E. (1974). Management Guide to Loss Control. International Loss Control Institute. (Based on Bird's 1969 ICNA study of 1,753,498 accident reports.)
- Occupational Safety and Health Act of 1970. Pub. L. 91–596. United States Congress.
- Health and Safety at Work etc. Act 1974. c. 37. UK Parliament.
- Reason, J. (1990). Human Error. Cambridge University Press.
- Dekker, S. (2006). The Field Guide to Understanding Human Error. Ashgate.
- Hollnagel, E., Wears, R.L. & Braithwaite, J. (2015). From Safety-I to Safety-II: A White Paper. University of Southern Denmark / University of Florida / Australian Institute of Health Innovation.
- Leso, V., Fontana, L. & Iavicoli, I. (2018). The occupational health and safety dimension of Industry 4.0. La Medicina del Lavoro, 110(5), 327–338.
- Manuele, F.A. (2011). Reviewing Heinrich: Dislodging two myths from the practice of safety. Professional Safety, 56(10), 52–61.
- European Commission (2021). EU Strategic Framework on Health and Safety at Work 2021–2027. COM(2021) 323 final.
NOTE: AI (Claude Opus 4.7) was used whilst curating parts of this edition. All opinions are my own.


Responses